¶ GHRP-6: Benefits, Dosage, & Side Effects
| Sequence | His-D-Trp-Ala-Trp-D-Phe-Lys-NH2 |
| Formula | C46H56N12O6 |
| Molar Mass | 873.01 g/mol |
| Category | GH Secretagogue (GHS) |
| Half-life | ~20-30 mins (Plasma) |
| Admin | Subcutaneous Injection |
| FDA Status | Not Approved / Banned for Compounding |
| CAS | 87616-84-0 |
GHRP-6 (Growth Hormone-Releasing Peptide-6) is a synthetic hexapeptide that robustly stimulates the release of growth hormone (GH) by mimicking the hunger hormone ghrelin. While effective for restoring GH levels, its use in longevity protocols has been largely superseded by newer analogs like Ipamorelin due to GHRP-6's significant appetite-stimulating side effects and recent FDA restrictions on compounding.
¶ At a glance
Aliases
- Also known as: Growth Hormone-Releasing Hexapeptide, SKF-110679
- Amino acid sequence: His-D-Trp-Ala-Trp-D-Phe-Lys-NH2
- Sequence length: Hexapeptide (6 amino acids)
- Category: Growth Hormone Secretagogue (GHS), Ghrelin Mimetic
Key points
- Strongest Benefit: Potent, pulsatile release of growth hormone (GH), which can aid in recovery and body composition.
- Notable Effect: Causes intense, rapid-onset hunger ("ghrelin hunger") due to activation of hypothalamic ghrelin receptors.
- Key Limitation: Short half-life requires multiple daily injections; significant cross-reactivity with cortisol and prolactin at higher doses.
- Safety/Legal: Placed on the FDA's Category 2 list (late 2023), making it effectively illegal for U.S. pharmacies to compound.
What people use it for
- Main goals: Muscle growth (bulking), appetite stimulation (for those struggling to eat), injury recovery, and anti-aging (GH restoration).
- Evidence quality (overall): Moderate for GH secretion; Low for long-term longevity outcomes.
¶ Legal & regulatory status
As of late 2023/2024, the FDA placed GHRP-6 on the Category 2 list of bulk drug substances (substances with significant safety risks). This classification effectively prohibits U.S. compounding pharmacies (503A and 503B) from producing GHRP-6. Legitimate access via telemedicine has largely ceased.
Regulatory classification
- FDA status: Unapproved. GHRP-6 is not an FDA-approved drug for any indication.
- Prescription requirement: It was previously available via prescription from compounding pharmacies, but this pathway is now closed in the U.S.
- DEA schedule: Not a controlled substance (unscheduled), but sale for human consumption is restricted under the FD&C Act.
Geographic legal status
- United States: Banned for compounding. Possession for research purposes is generally not criminalized for end-users, but sale for human use is illegal.
- International: Varies. Generally considered a prescription-only substance or research chemical in the UK, Canada, and Australia.
Sports and competition
- WADA status: Prohibited. Listed under S2. Peptide Hormones, Growth Factors, Related Substances, and Mimetics. Banned at all times (in and out of competition).
Source quality considerations
- With the compounding ban, users are forced to rely on "research chemical" vendors. These sources are unregulated, raising significant risks regarding purity, heavy metal contamination, and under-dosing.
¶ What is GHRP-6?
GHRP-6 is one of the first synthetic Growth Hormone Secretagogues (GHS) developed. Unlike Growth Hormone Releasing Hormone (GHRH), which is endogenous to the human body, GHRP-6 is a synthetic met-enkephalin analog designed specifically to stimulate the pituitary gland.
- Definition: A synthetic hexapeptide (6 amino acids) containing non-natural D-amino acids (D-Trp, D-Phe) to improve stability and receptor binding.
- Mechanism Class: It is a ghrelin mimetic. It binds to the Ghrelin Receptor (GHS-R1a).
- Development History: Developed in the 1980s, effectively predating the discovery of the hormone ghrelin itself (1999). Researchers found the peptide stimulated GH before they knew the natural ligand (ghrelin) existed.
- Key Property: It induces a massive, immediate "pulse" of GH secretion, independent of the body's natural GHRH signal, although it works best when GHRH is also present.
¶ What are GHRP-6's main benefits?
Most evidence for GHRP-6 comes from acute physiological studies measuring hormone release, rather than long-term clinical trials on disease outcomes.
1. Growth Hormone Restoration
- Outcome: Rapid, high-amplitude elevation of plasma Growth Hormone (GH).
- Magnitude: Large. Studies show it can elevate GH levels in elderly subjects to those seen in young adults[1].
- Evidence Quality: High. Replicated in numerous human trials.
2. Body Composition (Muscle & Fat)
- Outcome: Potential increase in lean body mass (LBM) and decrease in fat mass.
- Direction: Positive (↑ LBM, ↓ Fat).
- Caveat: While GH elevation is known to improve body composition, the strong appetite-stimulating effect of GHRP-6 often leads to increased caloric intake, which can negate fat loss efforts ("dirty bulking").
- Evidence Quality: Low. Direct RCTs on GHRP-6 monotherapy for body composition are scarce; most data is inferred from general GH therapy or animal models.
3. Appetite Stimulation
- Outcome: Significant increase in hunger.
- Mechanism: Direct activation of hypothalamic ghrelin receptors.
- Utility: clinically useful for cachexia (wasting), sarcopenia in the elderly, or failure to thrive, but often a side effect for general anti-aging users.
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| GH Secretion | High | High | 10+ | Acute bolus studies in healthy & elderly adults; robust pulses confirmed[1:1][2]. | |
| Appetite | ↑↑ (n/p) | High | Moderate | 5+ | Effect is immediate (20 mins post-injection); useful for wasting, negative for diet control. |
| Lean Body Mass | ↑ (?) | Moderate | Low |  |
Inferred from GH data; specific GHRP-6 body comp trials in humans are rare/small. |
| Sleep Quality | Moderate | Low | 2 | Enhances Stage 2 sleep and pulsatility during night[3]. |
** Consistency: High (most studies agree).
*** Trials: Approximate number of relevant human studies.
¶ How does GHRP-6 work?
GHRP-6 operates via a distinct pathway from the body's natural Growth Hormone Releasing Hormone (GHRH).
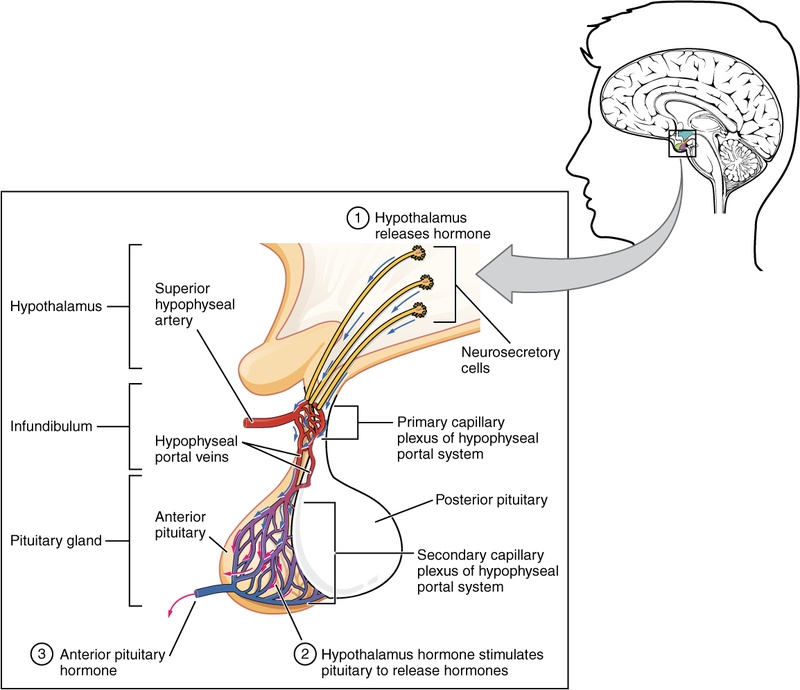
1. The Ghrelin Pathway (GHS-R1a)
- GHRP-6 binds to the Growth Hormone Secretagogue Receptor 1a (GHS-R1a) in the pituitary and hypothalamus.
- This is the same receptor targeted by the "hunger hormone" ghrelin.
- Activation triggers a Phospholipase C (PLC) signaling cascade, releasing calcium stores that cause pituitary cells (somatotrophs) to dump their stored growth hormone.
2. Pulsatile vs. Continuous Release
- Pulsatile: GHRP-6 induces a specific "pulse" or spike in GH. This mimics the body's natural rhythm better than synthetic HGH (which provides a steady/flat baseline if not timed perfectly).
- Synergy: Because it acts on a different receptor than GHRH, combining GHRP-6 with a GHRH analog (like CJC-1295) creates a synergistic effect.
- GHRH = "Turns on the faucet" (increases production).
- GHRP-6 = "Opens the floodgates" (triggers release).
- Result: A GH release greater than the sum of the two parts.
Pharmacokinetics
- Half-life: Very short (~20-30 minutes).
- Bioavailability: Zero orally (destroyed by digestion). Must be injected.
- Clearance: Rapidly cleared by the liver and kidneys.
¶ Effects on different systems
Metabolic Health
- GHRP-6 increases IGF-1 (Insulin-like Growth Factor 1) via the GH axis, which drives protein synthesis and glucose uptake in muscle.
- Risk: It can temporarily increase blood glucose and, if used chronically at high doses, may contribute to insulin resistance (a known effect of elevated GH).
Musculoskeletal System
- The downstream release of IGF-1 promotes collagen synthesis and tissue repair.
- Anecdotal reports heavily favor GHRP-6 for "bulking" phases in bodybuilding due to the combination of anabolic hormones (GH/IGF-1) and caloric surplus (increased appetite).
Cardiovascular Health
- Some animal research suggests cardioprotective effects, particularly in reducing damage from ischemia or cardiotoxic drugs (like doxorubicin)[4]. However, human data in this specific domain is lacking.
¶ Administration, reconstitution, and storage
Routes of administration
- SubQ (Subcutaneous): The standard and most effective method. Injected into body fat (belly or thigh) using an insulin syringe.
- Intranasal: Available but significantly less bioavailable; requires much higher doses.
Reconstitution
- Diluent: Bacteriostatic Water (water with 0.9% benzyl alcohol) is required to keep the solution sterile for multiple doses.
- Volume: typically 1mL or 2mL of water is added to a 5mg vial.
- Handling: Peptides are fragile. Do not shake the vial; gently swirl until dissolved.
Example Reconstitution Math (5mg Vial)
- If you add 2mL of water to a 5mg vial:
- Concentration = 2.5mg/mL (2500mcg/mL).
- Dose (100mcg) = 0.04 mL (4 units on an insulin syringe).
- Dose (200mcg) = 0.08 mL (8 units on an insulin syringe).
Storage
- Powder (Lyophilized): Store in freezer (-20°C). Stable for years.
- Liquid (Reconstituted): Must be stored in the refrigerator (2-8°C). Use within 4-6 weeks to ensure potency.
¶ Dosage and protocols
Standard Dosing (Saturation Dose)
- Dose: 100 mcg per injection.
- Note: Doses above 100mcg yield diminishing returns for GH release (saturation point) but significantly increase side effects (cortisol/prolactin).
- Frequency: 2-3 times daily (e.g., Morning, Post-workout, Bedtime).
- Timing: Strictly on an empty stomach.
- 1 hour before food or 2 hours after food.
- Reason: Elevated blood sugar or insulin blunts the GH pulse.
Common Stacks
- The "Synergy" Stack: GHRP-6 (100mcg) + CJC-1295 No DAC (100mcg).
- This combination is the gold standard for maximizing GH pulse amplitude.
- The "Bulking" Stack: GHRP-6 is rarely used for cutting due to hunger. It is often used alone or with testosterone for mass gain phases.
Cycling
- Duration: Typically 8-12 weeks.
- Washout: A break of 4 weeks is often recommended to prevent receptor downregulation (desensitization), although pulsatile use mitigates this risk compared to continuous infusion.
¶ Safety and side effects
Common Side Effects
- Extreme Hunger: Occurs 15-30 minutes post-injection. Can lead to binge eating.
- Water Retention: Common early in the cycle (edema).
- Tingling/Numbness: Often felt in hands/wrists (carpal tunnel-like symptoms) due to fluid retention compressing nerves.
- Lethargy: A "crash" or sleepiness after the GH pulse.
Endocrine Side Effects (The "Spillover")
- Unlike more selective analogs (Ipamorelin), GHRP-6 is "messy." At high doses, it stimulates:
- Cortisol: The stress hormone (can cause anxiety, water weight).
- Prolactin: Can cause nipple sensitivity or gynecomastia in sensitive men.
Who should avoid it?
- Cancer Patients: GH/IGF-1 promotes cell growth; theoretical risk of accelerating tumor growth.
- Diabetics: GH can increase blood glucose and insulin resistance.
- Post-Traumatic Stress (PTSD): Ghrelin signaling is linked to fear/stress processing; some users report anxiety.
¶ Drug and supplement interactions
- Insulin / Carbs / Fats: All of these blunt the GH release. Do not take GHRP-6 with food.
- Glucocorticoids: May inhibit the efficacy of GH therapy.
- Somatostatin: The natural "brake" on GH. Choline supplements (like Alpha-GPC) are sometimes used to inhibit somatostatin and boost the GH pulse, though evidence is mixed.
¶ Cost considerations
- Historical Cost: Was relatively cheap compared to rHGH (Recombinant Human Growth Hormone).
- Current Status: Since the FDA compounding ban, price varies wildly in the gray market.
- Value Proposition: Low. Newer peptides like Ipamorelin offer the same GH benefits without the cortisol/prolactin issues and with less hunger, often for a similar price. GHRP-6 is now largely considered obsolete except for those specifically seeking appetite stimulation.
¶ Practical questions (FAQ)
1. Is GHRP-6 better than Ipamorelin?
Generally, no. Ipamorelin is much more selective (no cortisol/prolactin elevation) and does not cause extreme hunger. GHRP-6 is only superior if you want the hunger effect (e.g., for bulking or combating poor appetite).
2. Can I inject GHRP-6 with food?
No. It will not work. Fats and carbohydrates trigger somatostatin release, which blocks the GH pulse. You must be fasted.
3. Will GHRP-6 show up on a drug test?
Yes, if it is a WADA/sports anti-doping test (it is a banned substance). It does not show up on standard employment 5-panel drug screens.
4. Why was it banned for compounding?
The FDA cited safety concerns regarding the lack of sufficient data on long-term safety, potential adverse effects on blood sugar, and the availability of FDA-approved alternatives (like sermorelin or recombinant HGH for specific conditions).
¶ How we evaluated the evidence
We prioritized human clinical data involving GH secretagogues.
- GH Secretion Claims: Based on seminal pharmacokinetic studies (Smith et al., Thorner et al.) demonstrating robust GH release in humans.
- Body Composition Claims: Graded as Low Certainty due to the lack of direct RCTs isolating GHRP-6 (most data is confounded by stacks or extrapolated from HGH).
- Safety: Based on both clinical reports (cortisol/prolactin data) and extensive patient-reported outcomes from the peptide community over 20+ years.
¶ References
Smith RG, Thorner MO. Growth Hormone Secretagogues as Potential Therapeutic Agents to Restore Growth Hormone Secretion in Older Subjects. J Gerontol A Biol Sci Med Sci. 2003. https://pubmed.ncbi.nlm.nih.gov/14570870/ ↩︎ ↩︎
Popovic V, et al. The secretagogue effect of growth hormone-releasing peptide-6 on the pituitary-thyroid axis in healthy men. Clin Endocrinol. 1996. https://pubmed.ncbi.nlm.nih.gov/8881909/ ↩︎
Frieboes RM, et al. Growth hormone-releasing peptide-6 stimulates sleep, growth hormone, ACTH and cortisol secretion in normal man. Neuroendocrinology. 1995. https://pubmed.ncbi.nlm.nih.gov/7734029/ ↩︎
Berlanga-Acosta J, et al. Growth hormone releasing peptide-6 (GHRP-6) prevents doxorubicin-induced myocardial damages. Front Pharmacol. 2024. https://www.frontiersin.org/journals/pharmacology/articles/10.3389/fphar.2024.1402138/full ↩︎