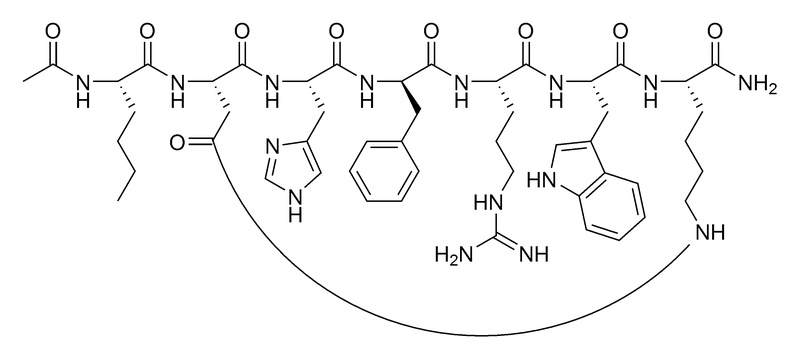
¶ Melanotan II
¶ At a Glance
| Feature | Specification |
|---|---|
| Classification | Synthetic Melanocortin Receptor Agonist (Peptide) |
| Primary Targets | MC1R (Pigmentation), MC4R (Libido/Appetite) |
| Primary Effects | Skin Tanning (Melanogenesis), Erectile Function, Libido Enhancement |
| Route | Subcutaneous Injection (Standard), Nasal Spray (Low Bioavailability) |
| Half-life | ~1–2 hours (Biological effects persist for days) |
| Status | Unapproved / Unregulated (Research Chemical) |
Melanotan II is not approved by the FDA, EMA, or TGA for human use. Development was halted in the early 2000s due to an unfavorable safety profile (severe nausea, hypertension). It is sold exclusively as an unregulated "research chemical." Users assume all risks regarding purity, sterility, and adverse effects.
¶ The Bottom Line
Melanotan II is a potent "lifestyle peptide" that reliably induces skin tanning and sexual arousal by mimicking the body's natural melanocyte-stimulating hormone. However, it carries a heavy side effect burden—most notably severe nausea, facial flushing, and the darkening of moles. While effective, its safety margin is narrow, and unregulated use has been linked to rare but serious toxicities like rhabdomyolysis and renal injury.
¶ Protocols and Dosage
1 mg = 1000 mcg.
Standard vials contain 10 mg.
¶ Clinical Trial Dosage (Historical)
In early pilot studies, the dose used was 0.025 mg/kg (25 mcg/kg) subcutaneous injection[1][2].
- For a 80 kg (176 lb) person: 2000 mcg (2 mg).
- Outcome: This dose caused severe nausea and vomiting in the majority of subjects, leading to the abandonment of this dosing strategy.
¶ Common "User" Protocols (Harm Reduction)
To mitigate the severe nausea observed in clinical trials, users in the "gray market" community have developed titration protocols that use much lower doses.
¶ 1. The "Loading" Phase (Acclimatization)
- Goal: To build tolerance to nausea and stimulate initial melanin production.
- Dose: 100 mcg to 250 mcg daily or every other day.
- Timing: Often taken immediately before bed to sleep through the initial nausea.
- Duration: 7–14 days, or until desired skin tone is approached.
¶ 2. The "Maintenance" Phase
- Goal: To maintain pigmentation with minimal compound exposure.
- Dose: 500 mcg once or twice a week.
- Context: Often timed 30 minutes prior to UV exposure (sun or solarium) to maximize the melanogenic response.
¶ 3. Nasal Spray Protocol
- Bioavailability: Very low (~30–40%) and highly variable[3].
- Dose: Users typically double or triple the injectable dose to achieve similar effects, often taking 1000 mcg (1 mg) or more per administration.
- Risk: The variability in nasal absorption can lead to accidental overdose if the mucosa is inflamed or if permeation is unexpectedly high.
¶ Benefits and Effects
¶ 1. Skin Pigmentation (Tanning)
Melanotan II is a super-potent agonist of the MC1 Receptor on melanocytes. It stimulates the production of eumelanin (brown/black pigment) even in the absence of UV light.
- Mechanism: Direct stimulation of melanogenesis.
- Result: Deep darkening of the skin, often described as a "dirty tan" due to the simultaneous darkening of moles, freckles, and lips.
- Protection: Increased eumelanin provides some photoprotection against UV damage, though this benefit is often negated by users intentionally seeking UV exposure to accelerate the process.
¶ 2. Sexual Function and Libido
Through activation of the MC4 Receptor in the central nervous system (hypothalamus), Melanotan II acts as a potent aphrodisiac and erectogenic agent.
- Outcomes:
- Men: Spontaneous erections occurring 1–5 hours post-injection (observed in 80% of subjects in trials)[2:1].
- Women: Increased genital arousal and desire.
- Distinction from Viagra: Unlike PDE5 inhibitors (Viagra/Cialis) which work mechanically on blood flow, Melanotan II works centrally on the brain's sexual processing centers.
¶ 3. Appetite Suppression
Activation of MC4R also regulates energy homeostasis. Many users report a significant reduction in appetite and cravings, particularly during the loading phase.
¶ Reality Check: The "Barbie Drug" Risks
While the benefits are reliable, the "cost" of using Melanotan II is significant.
¶ 1. The Nausea Barrier
Nausea is the most common side effect, affecting 60–80% of users in clinical trials[1:1]. It is centrally mediated (brainstem) and can range from mild queasiness to severe vomiting. It often subsides after consistent use but re-emerges if the dose is increased.
¶ 2. The "Mole" Issue
Melanotan II does not just tan the background skin; it darkens everything.
- Moles & Freckles: Existing moles will become darker and new moles ("eruptive nevi") may appear almost overnight.
- Hyperpigmentation: Areas of high melanin concentration (lips, scars, genitals) may become disproportionately dark.
¶ 3. The Quality Roulette
Because Melanotan II is illegal to sell as a supplement or drug, it is manufactured exclusively in unregulated underground labs.
- Purity: Vials often contain synthesis impurities (trifluoroacetic acid, truncated peptides).
- Label Claims: A "10 mg" vial may contain 5 mg, 15 mg, or no active ingredient at all.
- Mannitol: Often bulked with mannitol, which is harmless, but makes visual estimation of quantity impossible.
¶ Mechanism of Action
Melanotan II is a non-selective agonist of the melanocortin receptors (MCRs), exhibiting higher potency than the body's natural -MSH.
| Receptor | Primary Location | Function | MT-II Potency |
|---|---|---|---|
| MC1R | Skin (Melanocytes) | Pigmentation (Eumelanin synthesis) | High |
| MC3R | Brain, Gut | Energy homeostasis | Moderate |
| MC4R | Brain (Hypothalamus) | Sexual function, Appetite, Sympathetic tone | Superagonist (High Affinity) |
| MC5R | Exocrine Glands | Sebum production | Moderate |
The "PT-141" Connection:
Development of Melanotan II was abandoned because it stimulated both MC1R (tanning) and MC4R (sex/nausea). Scientists modified the molecule to create Bremelanotide (PT-141), which retains the MC4R effects (for libido) but has significantly reduced activity at MC1R (no tanning), leading to its eventual FDA approval for hypoactive sexual desire disorder[4].
¶ Evidence and Clinical Data
Although never approved, Melanotan II underwent Phase I and II trials which provide high-quality data on its effects.
¶ Efficacy Data
- Tanning: In the pilot Phase I study by Dorr et al. (1996), 3 doses of 0.025 mg/kg administered over 1 week induced significant tanning in all subjects[1:2].
- Erectile Dysfunction: A double-blind crossover study (Wessells et al., 1998) in men with organic and psychogenic ED showed that Melanotan II produced erections in 80% of participants compared to 10–20% for placebo. The erections were often spontaneous and unrelated to visual sexual stimulation[2:2].
¶ Safety Data (Clinical Trials)
In the same trials, the adverse event profile was substantial:
- Nausea: 65% of subjects (severe in ~13%).
- Flushing: >50% (face and upper body).
- Yawning/Stretching: A specific "stretching syndrome" was noted in >40% of subjects, linked to central dopaminergic/melanocortinergic activation.
¶ Safety and Toxicology
Beyond the "standard" side effects, unregulated use has revealed serious toxicities not fully characterized in the short pilot trials.
¶ 1. Dermatological Risks (Melanoma?)
- Dysplastic Nevi: MT-II causes rapid changes in mole morphology (darkening, size increase), which complicates skin cancer screening.
- Melanoma Risk: There are case reports of melanoma in situ developing shortly after starting MT-II[5][6]. While MT-II increases photoprotective eumelanin, it also stimulates melanocyte proliferation. If a user has pre-existing dysplastic cells, MT-II might theoretically accelerate their transformation, especially when combined with high UV exposure (tanning beds).
¶ 2. Renal Infarction
A specific, severe complication involves kidney injury.
- Mechanism: MT-II can cause intense vasoconstriction and platelet aggregation.
- Case Report: A healthy 39-year-old male suffered a renal infarction (tissue death in the kidney) after using MT-II. Users reporting flank pain should seek immediate medical attention[7].
¶ 3. Rhabdomyolysis
Severe muscle breakdown has been documented, particularly in overdose.
- Case Report: A user who injected 6 mg (a massive dose) developed rhabdomyolysis (CPK >17,000) and sympathomimetic toxicity, requiring ICU care[8].
¶ 4. PRES (Posterior Reversible Encephalopathy Syndrome)
Rare cases of PRES—a neurological condition involving brain swelling and seizures—have been linked to the rapid blood pressure spikes caused by melanocortin agonists[9].
¶ 5. Priapism
Because of its potent central erectogenic effect, erections lasting longer than 4 hours (priapism) are a risk, potentially requiring surgical drainage to prevent permanent tissue damage[10].
¶ References
Dorr, R. T., Lines, R., Levine, N., et al. (1996). Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study. Life Sciences, 58(20), 1777-1784. https://pubmed.ncbi.nlm.nih.gov/8637402/ ↩︎ ↩︎ ↩︎
Wessells, H., Fuciarelli, K., Hansen, J., et al. (1998). Synthetic melanotropic peptide initiates erections in men with psychogenic erectile dysfunction: double-blind, placebo controlled crossover study. Journal of Urology, 160(2), 389-393. https://pubmed.ncbi.nlm.nih.gov/9679884/ ↩︎ ↩︎ ↩︎
Turbo Tan. (2025). Melanotan 2 Absorption: Injection vs Nasal Spray. https://turbo-tan.net/melanotan-2-absorption-injection-vs-nasal-spray-which-delivers-better-results/ ↩︎
Palatin Technologies. (2000). Discontinuation of Melanotan II and focus on PT-141. https://en.wikipedia.org/wiki/Melanotan_II ↩︎
Hjuler, K. F., & Lorentzen, H. F. (2014). Melanoma associated with the use of melanotan-II. Dermatology, 228(1), 34-36. https://pubmed.ncbi.nlm.nih.gov/24356073/ ↩︎
Cousen, P., Colver, G., & Helbling, I. (2009). Eruptive melanocytic naevi following melanotan injection. British Journal of Dermatology, 161(3), 707-708. https://doi.org/10.1111/j.1365-2133.2009.09362.x ↩︎
Peters, B., Hadimeri, H., Wahlberg, R., & Afghahi, H. (2020). Melanotan II: a possible cause of renal infarction: review of the literature and case report. CEN Case Reports, 9(2), 159-161. https://doi.org/10.1007/s13730-020-00447-z ↩︎
Nelson, M. E., Bryant, S. M., & Aks, S. E. (2012). Melanotan II injection resulting in systemic toxicity and rhabdomyolysis. Clinical Toxicology, 50(10), 1169-1173. https://pubmed.ncbi.nlm.nih.gov/23121206/ ↩︎
Kaski, D., Stafford, N., Mehta, A., et al. (2013). Melanotan and the posterior reversible encephalopathy syndrome. Annals of Internal Medicine, 158(9), 707-708. https://www.researchgate.net/publication/236642736_Melanotan_and_the_Posterior_Reversible_Encephalopathy_Syndrome ↩︎
Devlin, J., Pomerleau, A., & Foote, J. (2013). Melanotan II overdose associated with priapism. Clinical Toxicology, 51(4), 383. https://www.tandfonline.com/doi/full/10.3109/15563650.2013.784775 ↩︎