¶ Ipamorelin: Benefits, Dosage, & Side Effects
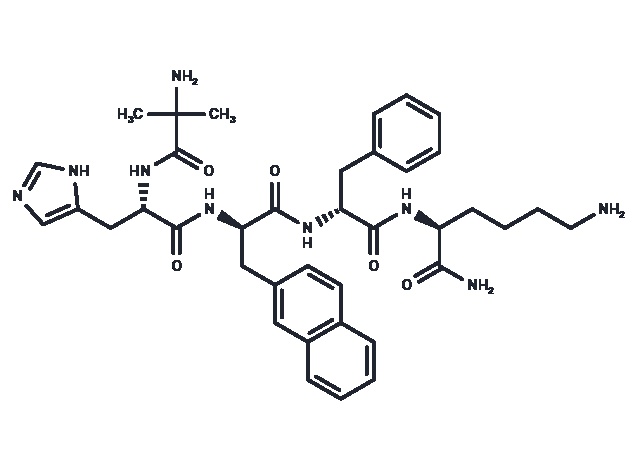
| Sequence | Aib-His-D-2-Nal-D-Phe-Lys-NH2 |
| Formula | C38H49N9O5 |
| Molar Mass | 711.85 g/mol |
| Category | GH Secretagogue (GHS) |
| Half-life | 2–3 hours |
| Admin | Subcutaneous (SubQ) |
| FDA Status | Not Approved (Restricted) |
| CAS | 170851-70-4 |
Ipamorelin is a synthetic pentapeptide and a highly selective agonist of the ghrelin/growth hormone secretagogue receptor. It is widely used in longevity and wellness circles to restore pulsatile growth hormone (GH) secretion, which naturally declines with age, without the significant side effects associated with older secretagogues or synthetic HGH.
¶ At a glance
Aliases
- Also known as: NNC 26-0161
- Amino acid sequence: Aib-His-D-2-Nal-D-Phe-Lys-NH2 (contains non-natural amino acids)
- Sequence length: Pentapeptide (5 amino acids)
- Category: Selective Growth Hormone Secretagogue (GHS)
Key points (high-level summary)
- Strongest Benefit: Ipamorelin safely stimulates the release of endogenous growth hormone in a physiologic, pulsatile manner, which may support recovery and body composition.
- Mechanism: Unlike GHRP-6 or GHRP-2, it is highly selective for GH release and does not significantly stimulate cortisol, ACTH, or prolactin (the "stress" and "water retention" hormones).
- Key Limitation: Human efficacy data for body composition (muscle growth/fat loss) is lacking; most evidence for these specific outcomes is extrapolated from animal models or other secretagogues.
- Safety: It has an excellent safety profile in humans, even at high doses, with no significant adverse events reported in clinical trials.
What people use it for
- Main goals: Anti-aging (GH restoration), improved recovery from exercise/injury, better sleep quality, and modest improvements in body composition (fat loss/muscle retention).
- Evidence quality (overall): Moderate for pharmacological effect (GH release); Low for long-term clinical outcomes (anti-aging/body comp).
¶ Legal & regulatory status
⚠️ CRITICAL INFORMATION: 2024 REGULATORY UPDATE
Regulatory classification
- FDA Status: Unapproved Drug. Ipamorelin is not FDA-approved for any medical condition in humans.
- Compounding Restrictions:
- In October 2024, the FDA's Pharmacy Compounding Advisory Committee (PCAC) voted against including Ipamorelin on the 503A Bulks List.
- Implication: This vote effectively recommends prohibiting compounding pharmacies from legally compounding Ipamorelin for patients. While previously available via prescription from wellness clinics, this channel is being rapidly closed.
- DEA Schedule: Not a controlled substance (unscheduled).
Geographic legal status
- United States: Legal to possess for research purposes; sale for human consumption is increasingly restricted due to FDA crackdowns on compounding.
- WADA Status: Prohibited. Ipamorelin is classified under Section S2 (Peptide Hormones, Growth Factors, Related Substances, and Mimetics) as a Growth Hormone Secretagogue. It is banned at all times (in and out of competition).
Source quality considerations
- Research Chemicals: Most users now access Ipamorelin via "research chemical" vendors. These products are labeled "Not for Human Consumption."
- Purity Risks: Third-party testing (HPLC/MS) is essential to verify purity (>99%) and net peptide content, as gray-market peptides may contain synthesis byproducts or heavy metals.
¶ What is Ipamorelin?
Ipamorelin is a synthetic pentapeptide (a chain of five amino acids) designed to mimic the action of ghrelin, the "hunger hormone." It binds to the Growth Hormone Secretagogue Receptor 1a (GHS-R1a) in the pituitary gland, triggering the release of stored growth hormone.
- Structure: It contains non-natural amino acids (Aib, D-2-Nal, D-Phe) which make it resistant to rapid degradation by enzymes like DPP-IV, giving it a longer half-life than native ghrelin.
- Selectivity: The defining feature of Ipamorelin is its selectivity. First-generation GHRPs (like GHRP-6) were "dirty" drugs that stimulated GH but also spiked cortisol (stress hormone) and prolactin (causing water retention/gynecomastia). Ipamorelin stimulates GH just as effectively but leaves these other hormones alone[1].
- Development: Originally developed by Novo Nordisk for the treatment of postoperative ileus (paralysis of the gut after surgery), it was abandoned for this indication due to lack of efficacy, but its potent GH-releasing properties were confirmed.
¶ What are Ipamorelin's main benefits?
Restoration of Growth Hormone Levels
Ipamorelin reliably restores serum GH and IGF-1 (Insulin-like Growth Factor 1) levels. In healthy adults, a single dose can trigger a significant pulse of GH within 40 minutes. This is the primary mechanism driving all downstream benefits.
Body Composition (Muscle & Fat)
- Outcome: Improved lean body mass and reduced adipose tissue.
- Evidence: Animal studies show clear increases in bone mineral content and muscle mass[2]. In humans, while direct RCTs for "bodybuilding" are absent, the mechanism (elevated GH/IGF-1) is well-established to promote lipolysis (fat breakdown) and protein synthesis.
- Reality Check: The effects are modest compared to exogenous HGH or anabolic steroids. It is more of a "preservation" and "optimization" tool than a mass builder.
Recovery and Repair
- Outcome: Accelerated healing of connective tissue and recovery from training.
- Mechanism: GH and IGF-1 are critical for collagen synthesis. Users frequently report faster recovery from soft tissue injuries and improved joint health.
- Outcome: Deeper, more restorative sleep.
- Mechanism: GH secretion is naturally tied to Slow-Wave Sleep (SWS). Users often report vivid dreams and a feeling of being more rested, although clinical data specifically measuring sleep architecture with Ipamorelin is limited.
¶ Evidence summary table (human outcomes)
| Outcome / Goal | Effect* | Consistency** | Evidence quality | Trials*** | Notes (population, duration, dose) |
|---|---|---|---|---|---|
| GH Release | High | High | 2+ | Robust dose-dependent GH release in healthy volunteers and post-op patients[1:1][3]. | |
| Safety (Short-term) | High | High | 2 RCTs | Well-tolerated even at massive doses (up to ~4mg daily) for 7 days[4]. | |
| GI Recovery (Ileus) | High | Moderate | 1 RCT | Failed to accelerate bowel recovery in post-op patients (n=114)[4:1]. | |
| Body Composition | Low | Very Low | 0 RCTs | No direct human RCTs measuring muscle/fat changes; extrapolated from animal data[2:1]. | |
| Bone Density | High | Low | 0 RCTs | Demonstrated in rats (longitudinal bone growth and mineral density)[2:2]; no human data. |
- Effect: ↑↑↑ = Strong Increase, ↔ = No Effect, ? = Unclear/No Data.
- Evidence Quality: High = Robust Human RCTs, Low/Very Low = Animal/Mechanistic data only.
¶ How does Ipamorelin work?
¶ Mechanism of Action
Ipamorelin acts as a key to unlock the pituitary gland's "GH store." It binds to the GHS-R1a receptor, initiating a signaling cascade (phospholipase C pathway) that causes the release of growth hormone vesicles.
¶ Pulsatile vs. Continuous: The Critical Difference
One of the most important concepts in GH therapy is the pattern of release.
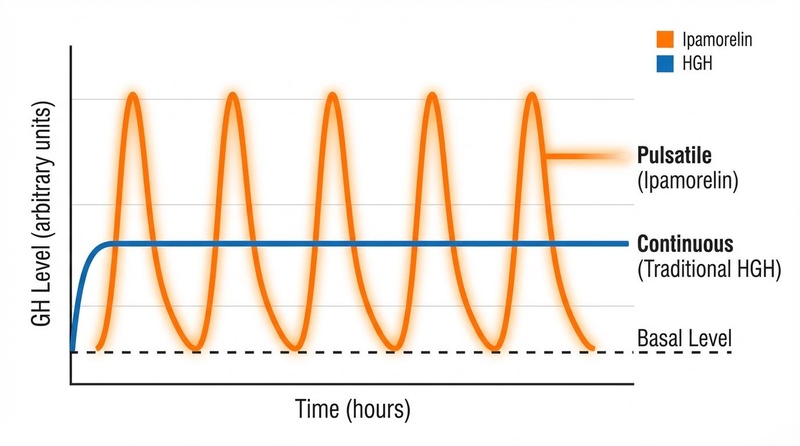
- Pulsatile (Ipamorelin): Creates a sharp "spike" of GH that lasts 2-3 hours and then falls to baseline. This mimics the body's natural rhythm.
- Benefit: Maintains insulin sensitivity and prevents receptor downregulation (tachyphylaxis).
- Continuous (Synthetic HGH): Often creates a sustained, flat elevation of GH.
- Risk: Constant exposure desensitizes receptors and can induce significant insulin resistance (diabetogenic effect).
¶ Pharmacokinetics
- Half-life: ~2–3 hours in humans. This short duration is what preserves the pulsatile nature but also necessitates daily dosing.
- Elimination: Cleared primarily through the liver and kidneys.
- Bioavailability: High subcutaneous bioavailability; poor oral bioavailability.
¶ Effects on different systems
¶ Metabolic Health
- Glucose/Insulin: Unlike HGH, Ipamorelin generally does not spike blood glucose or cause insulin resistance in healthy individuals because of its pulsatile nature. However, increasing GH always increases insulin resistance transiently (GH opposes insulin's action), so monitoring fasting glucose is recommended.
- Lipids: GH stimulates lipolysis (fat burning), particularly of visceral fat.
¶ Musculoskeletal System
- Bone: Animal studies suggest Ipamorelin increases bone mineral density (BMD) and bone growth velocity[2:3]. This makes it a potential candidate for addressing osteopenia or age-related frailty.
- Muscle: Supports the maintenance of lean mass (sarcopenia prevention) rather than massive hypertrophy.
¶ Skin & Appearance
- Collagen: GH/IGF-1 signaling is essential for fibroblast proliferation and collagen production. Anecdotal reports frequently mention "thicker" skin and improved elasticity, though cosmetic clinical trials are lacking.
¶ Administration, reconstitution, and storage
¶ Routes of administration
- Subcutaneous (SubQ): The gold standard. Injected into body fat (abdomen, thigh, glute) using an insulin syringe.
- Experience: Virtually painless due to the small needle (31G).
- Intranasal: Sprays exist but have significantly lower bioavailability (~10-20%), making precise dosing difficult and expensive.
- Oral: Not effective. The peptide is destroyed by stomach acid.
¶ Reconstitution (for lyophilized powder)
Ipamorelin is sold as a fragile white powder (lyophilized) that must be mixed with Bacteriostatic Water (water with 0.9% benzyl alcohol) to keep it sterile.
Example reconstitution (5mg vial):
- Add 2 mL of Bacteriostatic Water to the 5mg vial.
- Do not shake. Gently swirl until dissolved.
- Concentration: You now have 2.5 mg/mL (2500 mcg/mL).
Dosing Math (using the above 2.5 mg/mL mix):
- 100 mcg dose: 0.04 mL (4 units on insulin syringe)
- 200 mcg dose: 0.08 mL (8 units on insulin syringe)
- 300 mcg dose: 0.12 mL (12 units on insulin syringe)
Note: 100 units = 1 mL on a standard U-100 insulin syringe.
¶ Storage
- Powder: Freezer (-20°C). Stable for years.
- Reconstituted (Liquid): Refrigerator (2–8°C). Must be used within 3–4 weeks. Discard if it becomes cloudy or discolored.
¶ Dosage and protocols
¶ The "Clinical vs. Community" Discrepancy
There is a massive difference between doses used in safety trials and those used in practice.
- Safety Trials: Used massive doses (up to 4,000+ mcg daily) to prove safety.
- Community/Wellness: Uses much lower "saturation" doses (100–300 mcg) to mimic physiology.
¶ Standard "Anti-Aging" Protocol
- Dose: 100 mcg to 300 mcg per injection.
- Frequency: 1–2 times daily.
- Timing:
- Morning: Fasted, immediately upon waking.
- Night: Fasted, right before bed (mimics natural nocturnal spike).
- Fasting Rule: Crucial. Administer on an empty stomach (2 hours after food) and wait 20–30 minutes before eating. Insulin and somatostatin (released by food) blunt the GH spike.
¶ Cycling
- Common Cycle: 8–12 weeks ON, followed by 4 weeks OFF.
- Rationale: Although Ipamorelin causes less desensitization than GHRP-6, receptor sensitivity can still decline over months. Cycling ensures long-term efficacy.
¶ Safety and side effects
Ipamorelin is widely regarded as the "mildest" GH secretagogue.
Common side effects
- Injection site reactions: Mild redness or itching (histamine reaction).
- Headache: Often caused by the rapid pulse of GH or vasodilation. Usually subsides after the first week.
- Flushing: Warmth in the face/neck immediately after injection (~10-15 mins).
Less common / serious concerns
- Insulin Resistance: While safer than HGH, chronic elevation of GH/IGF-1 can still raise blood glucose.
- Water Retention: Rare with Ipamorelin (unlike GHRP-6), but possible at very high doses.
- Contraindications:
- Cancer: Active malignancy is a strict contraindication. GH and IGF-1 promote cell growth and can theoretically accelerate tumor growth.
- Pregnancy: Safety is unknown; avoid.
¶ Combining Ipamorelin with other peptides ("stacks")
¶ The Gold Standard: Ipamorelin + CJC-1295
This is the most popular peptide stack in existence.
- CJC-1295 (No DAC): A GHRH analog that amplifies the pulse.
- Ipamorelin: A GHRP that initiates the pulse.
- Synergy: Taken together, they create a GH pulse that is significantly larger than the sum of their individual effects.
- Protocol: Usually mixed in the same syringe (e.g., 100 mcg Ipamorelin + 100 mcg CJC-1295).
¶ Cost considerations
- Wellness Clinics (Prescription): Historically $200–$400 per month (includes supplies and oversight). Note: Availability is declining due to FDA restrictions.
- Research Chemicals: $30–$60 per 5mg vial.
- A 5mg vial at 200mcg/day lasts ~25 days.
- Monthly cost: ~$40–$70 (excluding shipping/supplies).
- Value: Generally considered high value because it provides many benefits of HGH therapy at a fraction of the cost (~10% of the cost of pharma HGH).
¶ Practical questions (FAQ)
1. Does Ipamorelin make you hungry?
No. Unlike GHRP-6 and GHRP-2, Ipamorelin does not significantly stimulate the hunger center in the hypothalamus. Most users report no change in appetite.
2. Will it show up on a drug test?
Standard employment drug tests do not look for peptides. However, it is banned by WADA and professional sports leagues. Sophisticated anti-doping labs can detect it.
3. Can I take it with food?
No. Food (especially carbs and fats) triggers insulin and somatostatin, which shut down GH release. You must be fasted for the peptide to work effectively.
4. How long does it take to see results?
- Sleep/Recovery: 1–2 weeks.
- Skin/Hair: 4–8 weeks.
- Body Composition: 12–24 weeks (combined with diet/training).
5. Is it safe for women?
Yes. Because it doesn't affect testosterone or induce virilization, it is popular among women. However, women are generally more sensitive to water retention and may start at lower doses (50–100 mcg).
¶ How we evaluated the evidence
We prioritized human clinical data for safety and pharmacokinetics. For efficacy (body composition), we acknowledged the lack of direct human RCTs and relied on mechanistic data and animal studies, clearly distinguishing these from proven human outcomes. We placed significant weight on the 2024 FDA PCAC proceedings to provide the most current regulatory context.
¶ References
Raun, K., et al. (1998). Ipamorelin, the first selective growth hormone secretagogue. European Journal of Endocrinology, 139(5), 552-561. https://pubmed.ncbi.nlm.nih.gov/9849822/ ↩︎ ↩︎
Svensson, J., et al. (2000). The GH secretagogues ipamorelin and GH-releasing peptide-6 increase bone mineral content in adult female rats. Journal of Endocrinology, 165(3), 569-577. https://joe.bioscientifica.com/view/journals/joe/165/3/569.xml ↩︎ ↩︎ ↩︎ ↩︎
Gobburu, J. V., et al. (1999). Pharmacokinetic-pharmacodynamic modeling of ipamorelin, a growth hormone releasing peptide, in human volunteers. Pharmaceutical Research, 16(9), 1412-1416. https://pubmed.ncbi.nlm.nih.gov/10496658/ ↩︎
Beck, D. E., et al. (2014). Prospective, randomized, controlled, proof-of-concept study of the Ghrelin mimetic ipamorelin for the management of postoperative ileus in bowel resection patients. International Journal of Colorectal Disease, 29(12), 1527-1534. https://pubmed.ncbi.nlm.nih.gov/25331030/ ↩︎ ↩︎